We have heard a lot lately about “alternative facts” and “fake news” but I have not heard any mutterings about these misgivings as it relates to the current opioid epidemic. But then again, despite the number of deaths being claimed every day by fentanyl and heroin and in contrast to the sound bites heard during the presidential primaries, no one is talking facts about addiction. For that matter, politicians are barely even talking about addiction! We are talking a lot about the murders caused by immigrants, and there is no one doubting that immigrants do murder people, but so do native born Americans, and at a much higher rate than first generation immigrants. So, yes, we need to be concerned why second generation immigrants commit crime at rates much higher than their forefather immigrants and at a rate similar to native-born Americans; but if we are really serious about saving lives, let’s also talk about that which claims more lives than gun crime or automobile accidents – the disease of addiction. Let's not get caught up in the fake news that building a great wall or cutting Medicaid funding and trashing the Affordable Care Act will stop the influx of drugs or assist those afflicted with the disease of addiction. I hope you will read on.
So what are the facts:
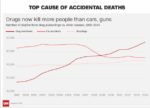
Drug overdoses now kill more Americans than guns
Overall, overdose deaths rose 11 percent last year, to 52,404. By comparison, the number of people who died in car crashes was 37,757, an increase of 12 percent. Gun deaths, including homicides and suicides, totaled 36,252, up 7 percent.
More than 50,000 Americans died from drug overdoses last year — the most ever.
The disastrous tally has been pushed to new heights by soaring abuse of heroin and prescription painkillers, a class of drugs known as opioids.
Heroin deaths rose 23 percent in one year, to 12,989, slightly higher than the number of gun homicides, according to government data released Thursday.
Deaths from synthetic opioids, including illicit fentanyl, rose 73 percent to 9,580
Overdose deaths rise by more than 100 percent in some states, CDC report says
According to data from the Centers for Disease Control and Prevention, 30 states saw increases in overdose deaths resulting from the abuse of heroin and prescription painkillers, a class of drugs known as opioids. New Hampshire saw a 191 percent increase while North Dakota, Massachusetts, Connecticut and Maine had death rates jump by over 100 percent.
Louisville, Kentucky reports record spike of 52 overdoses in 32 hours
“What we’re seeing in the streets right now is fentanyl mixed with heroin, as opposed to heroin mixed with fentanyl.”
“Everything happens for a reason, and I’m thankful it did happen, because I have a new look-out on life,” said Nathan Johnson, who said a recent overdose has him ready to stay clean. “They threw me in the shower, they did 18 minutes of CPR before the cops got there. Nothing was working, so the cop came in and he had to use two Narcans. It brought me back to life,” said Johnson. He can now use naloxone — or Narcan— on others. Kentucky’s ‘Good Samaritan’ law protects people who are administering the drug in an effort to keep someone alive.
“We’re often accused of being enablers, and we are. We are enablers. We enable people to live” said Read.
Heroin-related deaths increased 439% from 1999 to 2014. As of 2014, heroin-related deaths had more than tripled in five years and quintupled in 10 years.
Opioid Addiction – ASAM - 2016 Facts & Figures
Adolescents (12 to 17 years old)
- In 2015, 276,000 adolescents were current non-medical users of pain reliever, with 122,000 having an addiction to prescription pain relievers.
- In 2015, an estimated 21,000 adolescents had used heroin in the past year, and an estimated 5,000 were current heroin users. Additionally, an estimated 6,000 adolescents had heroin a heroin use disorder in 2014
Women
- Heroin overdose deaths among women have tripled in the last few years.
Trump leaves out context in claim about immigrants and crime
Overall, there are about 16,000 murders and 10,000 drunk driving deaths a year (the drunk driver is the person killed more than 60 percent of the time)
About 11.1 million unauthorized immigrants accounted for about 3.5% of the total national population in 2014, according to Pew Research Center. Certainly some undocumented immigrants do commit violent crimes
While Trump’s discourse suggests waves of immigrants equals violence, scholars say studies don’t substantiate that message.
Research on immigrants and crime finds that immigrants are not more likely than U.S.-born individuals to take part in crime, said Christopher P. Salas-Wright, an assistant professor at Boston University’s School of Social Work.
"Again and again, we see evidence that they are not," Salas-Wright said. "In fact, it’s the opposite."
Studies show that for the most part, people who migrate are a self-selecting group who want to better their lives, provide for their families back in their home countries and who don’t want to risk getting in trouble with the law, said Kubrin, the criminology professor at University of California, Irvine.
The American Immigration Council, a pro-immigrant nonprofit, analyzed data from the Census’ 2010 American Community Survey and found that about 1.6 percent of immigrant males between 18 and 39 years old were incarcerated, compared to 3.3 percent of the native-born population in that same age group. (The Census does not specify legal status.)
Justice Quarterly - An Examination of First and Second Generation Immigrant Offending Trajectories
Results suggest that the myth remains; trajectory analyses reveal that immigrants are no more crime-prone than the native-born. Foreign-born individuals exhibit remarkably low levels of involvement in crime across their life course. Moreover, it appears that by the second generation, immigrants have simply caught up to their native-born counterparts in respect to their offending. Implications of the findings for theory and future research are discussed.
Crime rises among second-generation immigrants as they assimilate

 I have included below a copy of the personal letter I received. I look forward to assisting the Surgeon General in his mission to destigmatize the disease of addiction! Remember - "It Takes a Village" and "A Thousand Points of Light".
I have included below a copy of the personal letter I received. I look forward to assisting the Surgeon General in his mission to destigmatize the disease of addiction! Remember - "It Takes a Village" and "A Thousand Points of Light".