I could not let this day pass without commenting on International Overdose Awareness Day. We repeatedly read in the media and listen to politicians about the cost of this and the cost of that. When was the last time you heard them speak about the cost of not dealing with the scourge to society called ADDICTION. If you want to believe it is a disease, or for that matter, just simply mind over matter, fine – but at least deal with the economics. The United States spends $193 Billion Dollars per year in dealing with the consequences of illicit drug use related to crime, lost work productivity and health care. If the consequences of abuse of tobacco and alcohol is included, cost rises to more than $700 Billion Dollars annually. Here's the link: Drug Abuse
So, please ask all your politicians, local and national, what they are doing to curb the financial costs of the disease of addiction. And then, direct them to the website: overdoseday.com and tell them to read the stories of lives lost and families devastated.
The following is a quote from International Overdose Awareness Day.
RETHINK & REMEMBER
International Overdose Awareness Day (IOAD) is a global event held on August 31st each year and aims to raise awareness of overdose and reduce the stigma of a drug-related death. It also acknowledges the grief felt by families and friends remembering those who have met with death or permanent injury as a result of drug overdose. Overdose Day spreads the message that the tragedy of overdose death is preventable.
The theme for 2015 is Rethink and Remember.
I hope with a “novel” approach, Addiction on Trial, will help to change hearts and minds about the scourge of addiction. We can do so much more to curb its devastating consequences and save lives and dollars.
After 10 weeks we are finally finished with blaming, but what a way to end – let’s blame our politicians and our other public officials. Why? - Because if all our public officials showed the leadership and courage of Vermont Governor Shumlin, we would have another solution to curb the heroin epidemic. As I stated in an Op-Ed in the Boston Globe:
There should be just as many public service announcements about addiction as there are Viagra and Cialis commercials. In addition, expansion of addiction treatment services in jails would help to mitigate much of the revolving door phenomenon. Furthermore, we should demand that our medical schools and hospitals improve addiction training of our physicians. While there is plenty of blame to go around, let's focus on the solutions. The scourge of addiction is in all of our yards. The solution is to decrease the demand with bold public initiatives and a change in attitude. It is both the humanitarian and fiscally responsible thing to do.
We need our politicians and public officials to stand up for what is right and bring forward the real facts about addiction. I explained this further in another Op-ed submitted to the Boston Globe:
We must cut back on the demand to stand a chance of limiting the financial damage. And to our politicians, I know this is a politically hot issue, but lives and dollars are at stake and it is time to lead the charge to educate through scientific fact and not out of fear. I commend Governor Shumlin of Vermont for spending his entire state of the state address on this essential economic issue and his call to attack the epidemic on the demand side (treatment); recognizing that putting more people in jail may make us feel good on the short term, but does not solve the problem. Governor LePage of Maine addressed the issue of drug addiction as an economic issue as well, but he unfortunately spoke not of increased funding for treatment and access to care, but only of expanded law enforcement and judicial response.
As the death of Philip Seymour Hoffman’s has again reinforced, drug addiction, including heroin abuse, is an equal opportunity disease affecting all socioeconomic strata; and knows no boundaries. This is not a problem of the welfare state or the poor or less fortunate. It is NOT NIMBY!! The disease is present in our impoverished neighborhoods as well as our wealthy suburban communities and in our resort towns and backwoods … Establishing treatment centers for addiction in one’s own locale should be worn as a badge of honor, no different than establishing a cancer treatment center or cardiac center; both of which are illnesses that may be related to the disease of addiction. NIMBY no longer works!
We can make great strides to solve the scourge of heroin addiction, but we need to stop blaming and put words into action. As I have discussed over the past ten weeks, there is plenty of blame to go around!
Addiction On Trial exposes many of the reasons why we have a heroin epidemic; Police Chief, François Bergeron, understood the political and emotional realities of heroin addiction. The story may be fiction, but it is based on medical, legal and political truths. IT IS TIME TO STOP BLAMING AND TIME TO START IMPLEMENTING SOLUTIONS! Thank you for continued interest in my blog site and I hope that Chief Bergeron’s insights will make a difference (Chapter 15):
Although Chief Bergeron had witnessed first-hand the increasing influx of drugs into not only his community but into all of Downeast Maine, Annette's death and the likelihood it was drug connected posed challenges never before encountered. Although the chief understood that drug addiction was a complicated topic and a burgeoning problem, this view was not shared by most, many of whom even refused to believe that Downeast Maine had a significant drug issue despite the fact that a methadone treatment center about two hours away had recently opened to treat the epidemic of heroin and Oxycontin addiction in the region. There had been a prolonged battle within the ranks of city government and among the citizens who irrationally opposed the siting of the treatment center, delaying its opening for years. Eventually, there was some acknowledgment that Downeast Maine, no different than innumerable regions and communities up and down the east coast, had a heroin and Oxycontin problem, but it was greatly minimized. The clinic was finally approved after much rancor, but treatment was initially limited to one hundred patients. Since no one ever wants to believe its municipality has a significant drug problem, it was decided that opening up one hundred outpatient slots would more than satisfy the need and help to quell the escalating controversy. The clinic filled all its patient slots within a month and droves of needy patients were placed on waiting lists.
This struggle to establish treatment centers was not unique. There were similar controversial and heated discussions in many cities and towns … Lawsuits between municipalities against well-intentioned medical providers were not unusual. Paradoxically, at about the same time, a New England Governor’s Council Forum had convened … Presentations by illustrious speakers demonstrated the extent of the epidemic …What Bergeron remembers most from the conference was the statement by a prominent elected official that “these are telling times when elementary and middle school children are offered a bag of 70-80 percent pure heroin for the price of a double scoop ice cream cone.” The forum’s mantra was interdiction, education, and treatment. This battle cry was good in theory, but in practice it was a different story at the local level. NIMBY—“Not In My Back Yard”—was the rallying cry of most municipalities. No town would admit to having a significant drug issue; it was always the next town over that had the problem. The rationale was based on the fear that if a drug addiction center was established in one’s own town, which of course did not have a problem to begin with, all the addicts from the neighboring townships would spread the scourge as they migrated for treatment, thereby creating a drug problem that never before existed. Despite the documented epidemic of drug abuse across the nation, hardly any individual town, if you spoke to the locals, had much of a problem.
Chief Bergeron understood the apprehension of the townsfolk, that a drug treatment center in West Haven Harbor would label the town as a drug haven. The tourists would be frightened and stay away, the local economy would falter, and everyone would suffer. As a result, many in need of treatment never got it. Chief Bergeron’s concern for the lack of treatment options was now a secondary issue. He recognized that the townsfolk's anger directed at an addict from away was irrational, especially before all the facts were known, but he also understood their desire for retribution for Annette's murder.
Thank you for coming back to my blog site. In case you have missed any of the previous eight blogs on the Ten Reasons for the Current Heroin Epidemic, please do scroll down to check them out. Today we will be discussing how Mental Health Treatment or actually the lack thereof has contributed to the overall increase in illicit drug and alcohol use, and opiate/heroin dependency.
It is well documented that patients with mental illness are still greatly underserved, and despite some positive movement to increase treatment funding and access, the drastic cuts from the distant and recent past have not been eliminated. NAMI, the National Alliance on Mental Illness, released the report State Mental Health Cuts: A National Crisis which documented the drastic cuts implemented by states between 2009 and 2011 for spending for children and adults living with serious mental illness. These cuts led to significant reductions in community and hospital based mental health services, with a direct effect also on access to psychiatric medications and crisis services. The Medicaid funding issue is a complex analysis, but there is no question that too many patients are left without viable treatment options. In an article by the Pew Charitable Trusts, Some States Retreat on Mental Health Funding, Medicaid expansion “may also have persuaded some states to pull back funding for community mental health centers and other mental health initiatives, including school and substance abuse programs.”
The lack of access is not limited to the Medicaid insured population, as many commercial insurers also do not cover mental health services in parity with medical and surgical illnesses. In addition to private insurance companies not abiding by parity laws, the federal and state governments, who are responsible for overseeing compliance, apparently are not doing a good job, Despite Laws, Mental Health Coverage Often Falls Short. It was also reported that “NAMI found that patients seeking mental health services from private insurers were denied coverage at a rate double that of those seeking medical services … [and] patients encountered more barriers in getting psychiatric and substance use medications.”
Enough with the statistics! How does this lead to the heroin epidemic? Simply stated, patients with mental illness are no different than patients with a wide variety of complaints – they all want to feel better. However, when there are roadblocks related to funding and access to treatment and medication for psychiatric illnesses, patients look elsewhere to feel better. It is a well-known phenomenon that patients who cannot access care are more likely to self-medicate. So it should not surprise us that patients with depression, anxiety, bipolar illness and other psychiatric health issues reach for drugs that make them feel better: alcohol, stimulants such as cocaine, and opioids such as OxyContin or heroin are commonly used.
When I started this blog series, I promised that I would not only assign blame for the Heroin Epidemic, but also offer solutions. So here is another solution: Federal and State Governments must enforce parity laws and we must increase access and funding for mental illness. As they say in the Midas commercial, “You can pay now or you can pay later, but you are going to pay.” Inadequate mental health treatment can lead to substance use, crime, dysfunctional family dynamics and an overall increase in financial costs to society.
Bad things can happen when mental illness goes untreated, and especially when drug use compounds the situation. In Addiction On Trial this is illustrated by Aunt Betty’s conversation with Jimmy’s father:
Adam continued, “Jimmy’s in jail. He was arrested for possession of drugs. But now they are trying to pin a murder on him, but there’s no proof, and well, it’s really a case of mistaken identity.” Adam tried to ground his runaway emotions, but with a trembling tone he blurted out what he so desperately wanted to believe. “Jimmy had nothing to do with it!”
Adam’s anxious moment gave Betty the opening she needed. “Adam, how can I help? And don’t lie to me. We both know that just because Jimmy may not have intended to do anything bad, well, you know what I am saying. When people are high on drugs, accidents happen and sometimes it looks like it wasn’t an accident.”
And during the trial, Venla Hujanen, the Finnish born District Attorney, also focuses on drugs and mental illness while cross examining Dr. Saul Tolson:
Dr. Tolson spoke softly while nodding affirmatively. The District Attorney proceeded, “So Dr. Tolson, it sounds like you do agree that if a person is addicted to drugs—even though he may have been ‘clean’ for a while, and even though when not using drugs he is able to process things better—if he returns to drug use and again becomes ‘high,’ his anger can resurface, poor choices can be made, and bad things can happen.”
As you may recall, the first blog in this series, Reason #1 for the Heroin Epidemic was “Blame the Doctors”. And now here we are again implicating the medical profession as a contributing factor. But this week I want to focus on the medical education process. To state it bluntly, Addiction Medicine training and emphasis on the complexity and interrelationship of addiction and underlying associated illnesses is lacking in our medical schools and residency programs. This not only leads to a lack of appreciation of the importance of screening patients for predisposition to and/or ongoing addiction, but also creates biases. In general, misconstruing of complex societal issues can lead to preconceptions that are not based in fact. When this hypothesis is applied to physicians who are asked to treat the difficult and the multifactorial aspects of addictive disease, bias can prevail. There are certain diseases that are more time consuming to manage than others, especially when the patient is either in denial and/or non-compliant. Examples may include Diabetes, Cardiac Disease and Lung Disease. But physicians in general receive the appropriate training to deal with the demands of these patients. That is not the case with addictive illnesses and bias is compounded by the other societal factors that influence perceptions, such as jailing patients (please see excerpt below).
However, inroads are being made to correct this deficiency. COPE (Coalition on Physician Education in Substance Use Disorders) is one such organization that is making great inroads within the medical educational process, and I felt honored to be chosen as a speaker at a recent event. I presented some facts such as:
The changing face of addiction now includes aging baby boomers and
heroin addiction is no longer just an inner city problem, as it has migrated to college campuses and to white suburban men and women in their late 20’s;
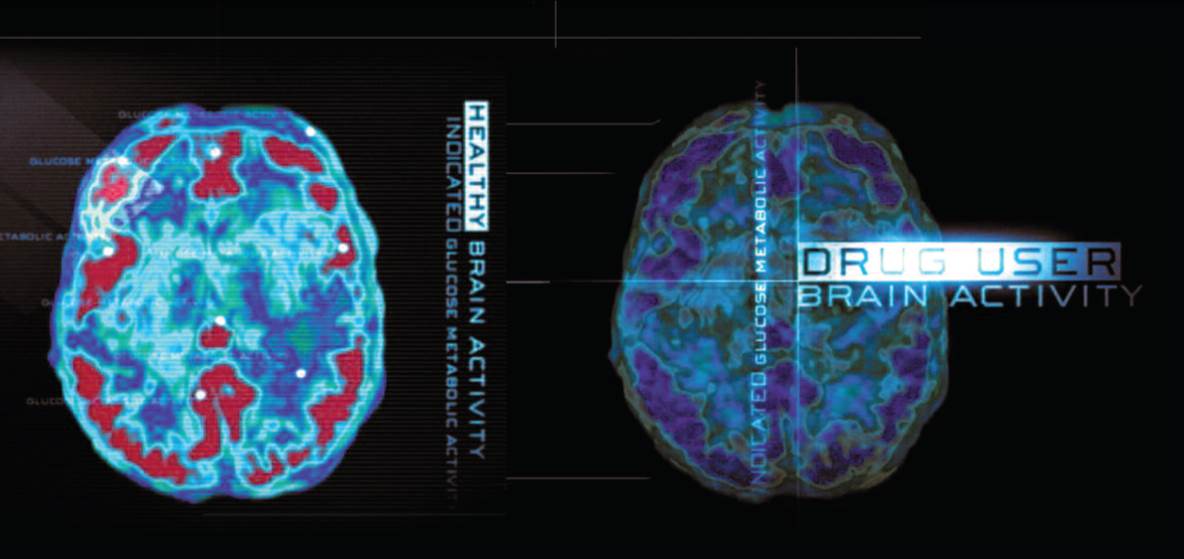
“Drug addiction is a brain disease that can be treated” (Nora D. Volkow, M.D., Director, National Institute on Drug Abuse)
Physician bias is another roadblock to solving the heroin epidemic, because biased doctors are less likely to treat patients with addiction, and as discussed in last week’s blog, it is essential to attack this scourge to society by decreasing demand through treatment and education. We need more doctors willing to treat patients and also to be more involved in educating our citizens and public officials that treatment works. Our medical schools and residency programs need to do more.
I am pleased that I have been asked by a medical school to use my book as a teaching tool to destigmatize the disease of addiction. And yes, it is time to stop jailing patients, as best discussed by Saul Tolson in the following excerpt from Addiction On Trial.
Pausing while attempting to make eye contact with each and every individual in the audience before proceeding, Dr. Tolson delivered his next few lines in a compassionate tone. “With no disrespect, but as a way to reinforce the point I am trying to make, I’d like to ask you to please tell me the difference between a nicotine or alcohol addict, who in some cases may even receive a heart or liver transplant, and someone addicted to heroin or cocaine? Why are those afflicted with the disease of addiction to certain drugs treated so differently than patients who suffer from nicotine or alcohol addiction or other chronic diseases like diabetes? Are they really any different?”
Dr. Tolson never relinquished the podium without one last attempt to convert the naysayers. “Now for those of you who fail to agree with me, and I know you’re out there, let me appeal to your wallets. To incarcerate one addicted patient—that’s right, jailing patients—costs between $40,000 and $50,000 per year. A one-year stay for a patient in a halfway house costs society about $20,000 per year and this does not include any medical care. But to treat one heroin addict as an outpatient with regular individual and/or group counseling sessions, ongoing urine drug testing to monitor for illicit drug use, a complete admission physical exam including laboratory tests that screen for contagious diseases such as Hepatitis C and HIV, and the daily monitoring of medication administration costs approximately $5,000 per year! That’s right—only $5,000 per year or about one-tenth the cost of putting this patient in jail!
Like they say in the Midas commercial, ‘you can pay now or you can pay later, but you’re gonna pay.’ Thank you all for your attention. I am able to stay for questions.”
Uncomfortable with the inevitable applause, Dr. Tolson kept repeating through the clapping, “So, there must be some questions.” The questions came, but none of his answers carried the consequences of those he would have to give to questions posed while under oath at the murder trial of James Frederick Sedgwick in Downeast Maine.
Welcome back to my addiction blog and I hope that as we discuss the final four reasons for the heroin epidemic, you will remember that there are solutions within reach. The issue of Supply & Demand directly relates to both the problem and the solution. Let me explain further.
Heroin production and distribution seems to be an unending saga; especially after the consequences of the War in Afghanistan. No matter how many drug lords and kingpins we kill or arrest, there is always someone willing to fill the void. Money and power is the “addiction” that attracts people to the illicit drug world. Interdiction and attempting to close our borders to drugs is a losing battle; and increasing tax payers’ burden by growing law enforcement and judicial budgets has been unsuccessful. Yes, we can arrest and incarcerate all the current drug pushers, big and small, and we can continue to burn the fields of the countries that produce opium; but the profits of this organized industry of drug production and distribution is so great that there is a continuously replenishable supply of people who want to be the next kingpin or the next local drug pusher.
Let’s look at this from a different perspective, using an economic analysis. If we cannot limit the supply, then we must look at the demand side of the equation. If there is decreasing demand, there will be decreasing profits and therefore decreasing production. I am not saying that we should abandon attempts to bring to justice those who are poisoning our communities with a constant flow of illicit drugs. What I am saying is we should attack the demand side of this problem with greater vigor. We spend $400 Billion Dollars annually dealing with the consequences of addiction. This should be incentive enough to advocate for more preventive programs and more treatment centers to decrease demand.
As I stated earlier in this blog series of the Ten Reasons for the Heroin Epidemic, there is plenty of blame to go around. We must focus on the solutions. The last blog dealt with NIMBY, which is interconnected with the Supply and Demand issue discussed today. Moving forward, over the next several weeks, we will address three more interrelated reasons and pose other solutions. I hope you will stay tuned for Reasons 8 - Physician Training & Biases; 9 - Mental Health Treatment and 10 - Public Officials.
Please enjoy the following excerpt from Addiction On Trial that gives insight into Jimmy’s inner struggles and I hope to see you next week.
What the defense team did not appreciate was the inappropriate loyalty one drug addict feels for another and the risks they will personally take to protect a drug-dependent comrade. As time went on, Jimmy would become more forthcoming, but a degree of brotherly protection persisted…
Jimmy struggled with this dilemma as it ripped away at his core, tossing and turning night after night in the confines of his cell until he felt soulless. He wished he could have just one session with his therapist. He dreamed, mumbling aloud as he conjured up Saul Tolson’s response.
“Saul, I just can’t tell on Travis…. His life is ruined. And then if I rat him out as the one who bought the heroin and the cocaine for Annette and me . . . I can’t do it! Just because he offered me the drugs, I didn’t have to use them. I knew better, or I should’ve. Damn it, if I could trade my life and bring back Annette and make Travis whole again, I’d do it. Why won’t they believe me?...
“Jimmy, I don’t think it’s that simple. And I think what you are saying is that you feel like you really let yourself down.”
Jimmy tossed in his hard cot, with sweat dripping off his body. “Oh, Saul, if I had a belt, I’d hang myself. I’ll never rat on Travis! Even if I did, who would believe me? I just can’t go on.” Jimmy let out a scream, “I want to die!”
“Hey keep the noise down. Just because you killed someone doesn’t mean you need to wake us all up. It’s three o’clock in the morning. If you want to die, then just go do it and shut up!”
Jimmy did not respond to the incarcerated voice a few cells away, but now fully awakened, Jimmy just laid there, crying softly to himself.